


Dr. Ho doesn't just direct dental animations — he treats dental patients. When he reconstructs the proximity of an implant to the inferior alveolar nerve, he knows exactly what the delivering clinician should have seen, measured, and done differently.


Nerve Injury — Lingual & Inferior Alveolar
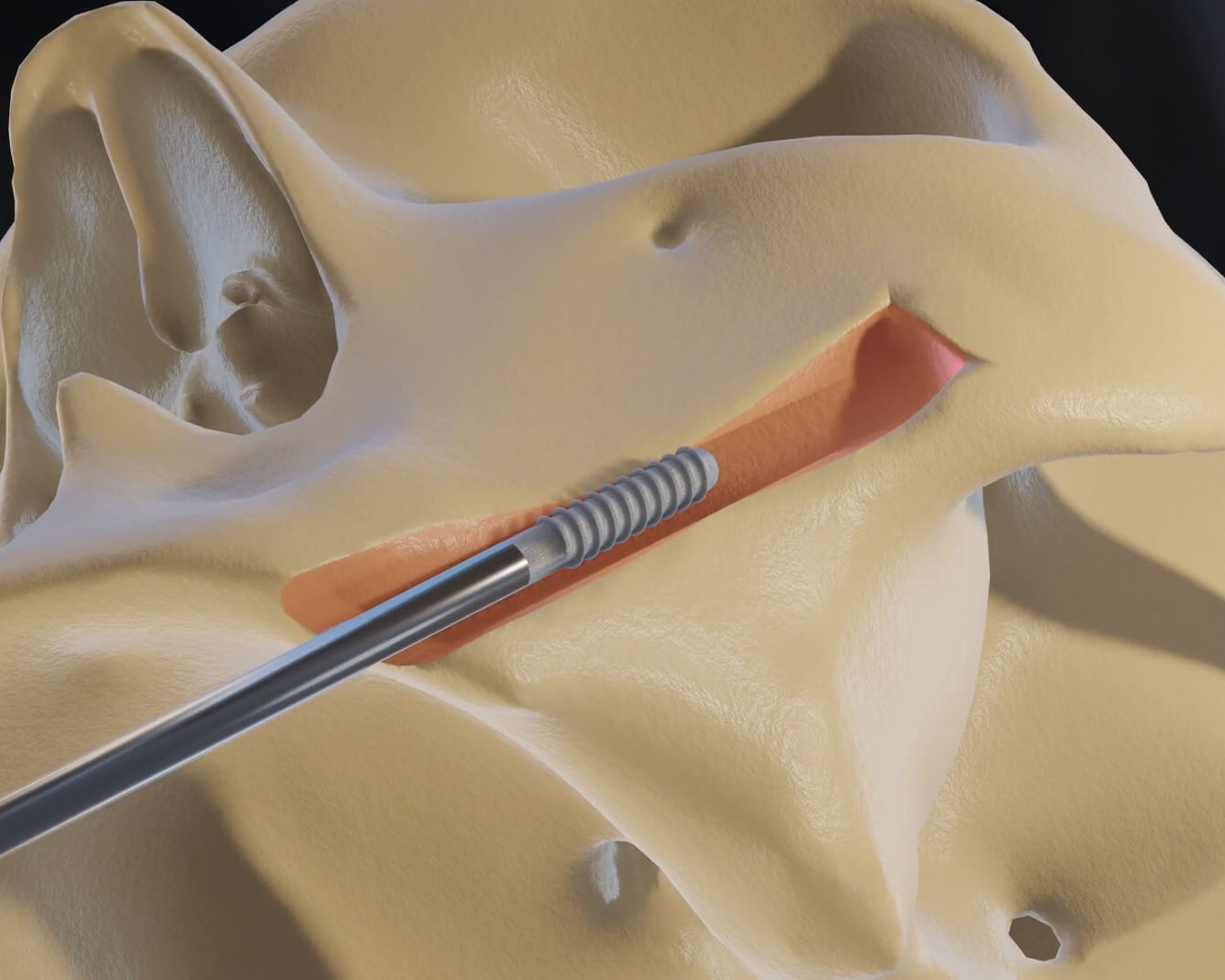
Show the Jury Exactly How Close the Drill Came to the Nerve — Using Your Client's Own CBCT Scan.
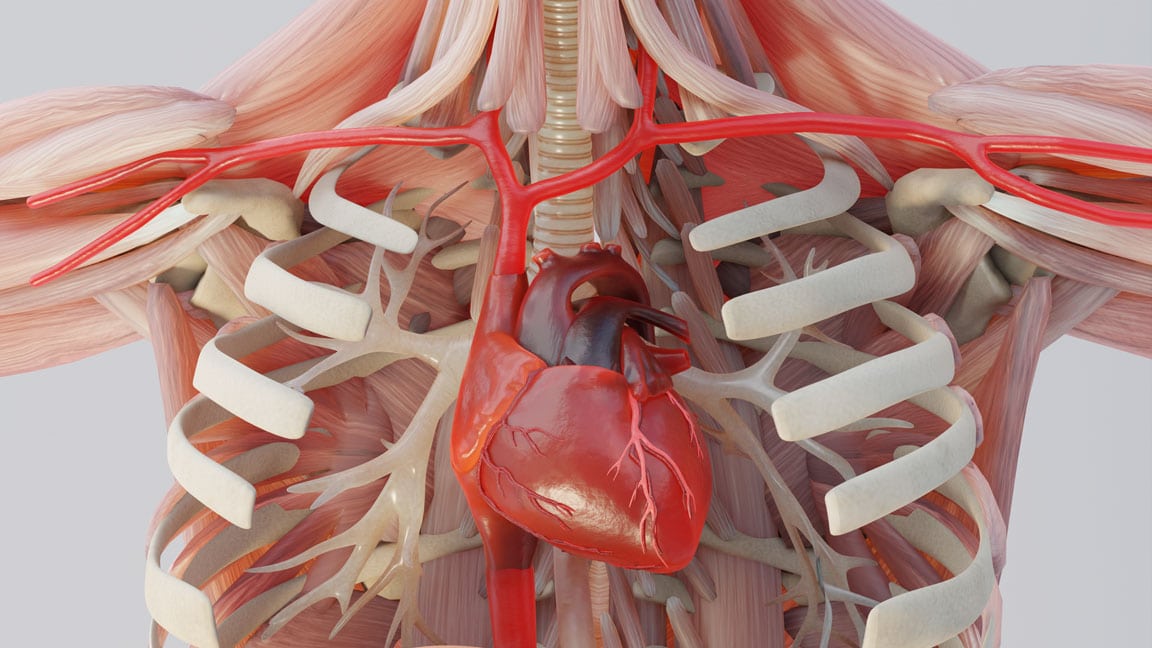
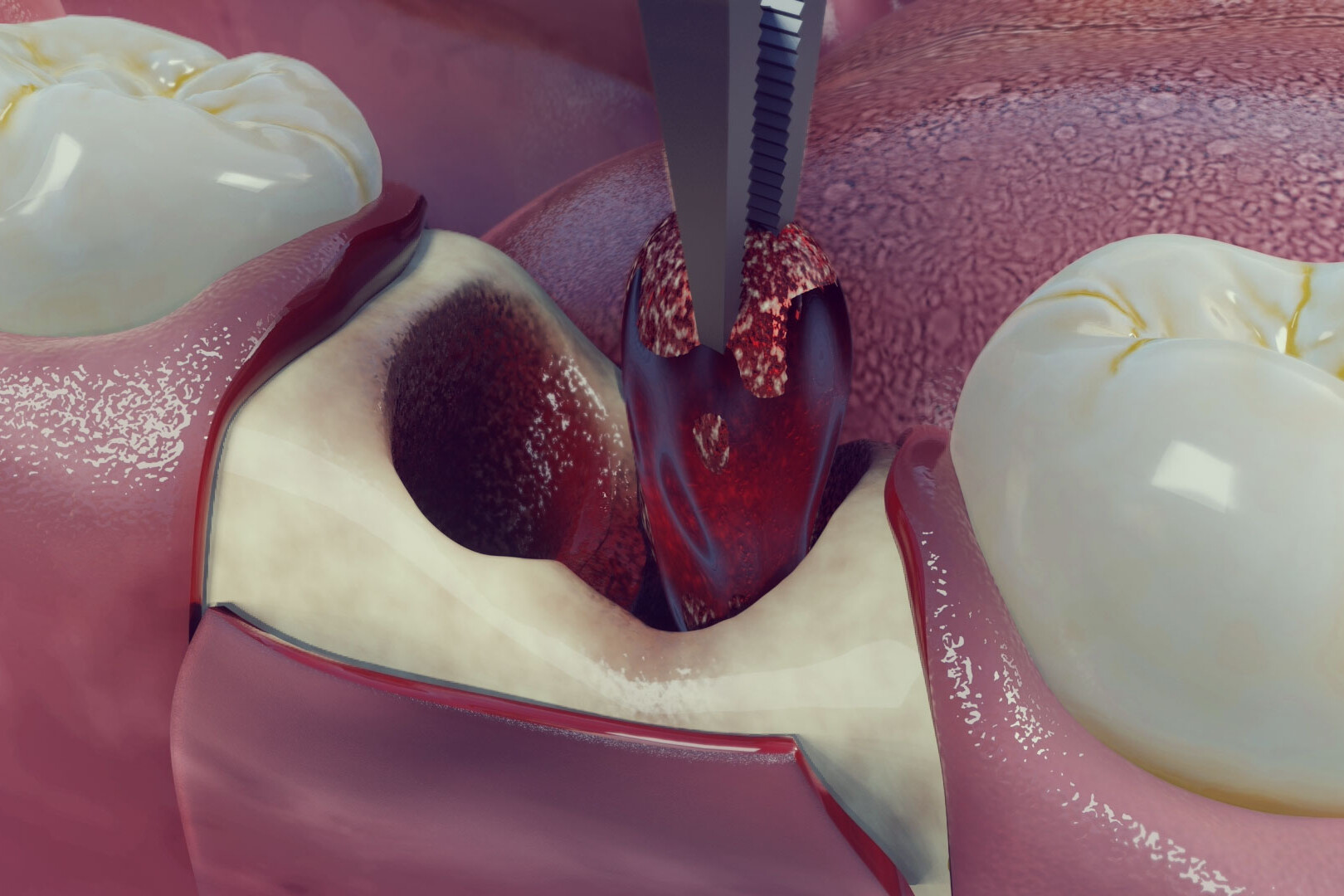
Inferior alveolar nerve and lingual nerve injuries are the most common and most contested dental malpractice claims. The defense argues the nerve position was anatomically variable and the injury was unforeseeable. We reconstruct the exact spatial relationship between the tooth roots, the surgical instrument, and the nerve canal using your client's pre-operative CBCT data — showing what a reasonably competent clinician would have measured, identified, and avoided. Nerve Injury (Lingual & Inferior Alveolar) CBCT-derived 3D reconstruction showing the precise location of the inferior alveolar canal or lingual nerve relative to the surgical site — rendered from your client's actual pre-operative imaging. The proximity that should have been identified on pre-surgical review becomes spatially undeniable. Your expert points to the measurement. The jury understands why it was negligent to proceed without nerve mapping or alternative technique. Standard of Care Comparison Side-by-side animation of the accepted pre-surgical nerve identification protocol and safe extraction or implant placement technique versus what the defendant actually performed — showing the specific departure from standard practice that caused the nerve injury. The deviation stops being an expert's opinion and becomes something the jury sees directly. Permanent Paresthesia & Dysesthesia We map the anatomical distribution of sensory deficit — the exact areas of numbness, tingling, or chronic pain your client experiences — back to the specific nerve injury documented in the imaging and clinical records. The connection between the procedural error and the permanent sensory consequence becomes a visual argument your expert can point to and the jury can follow without a dental degree.

Implant Failure, Bone Graft Complications & Sinus Perforation
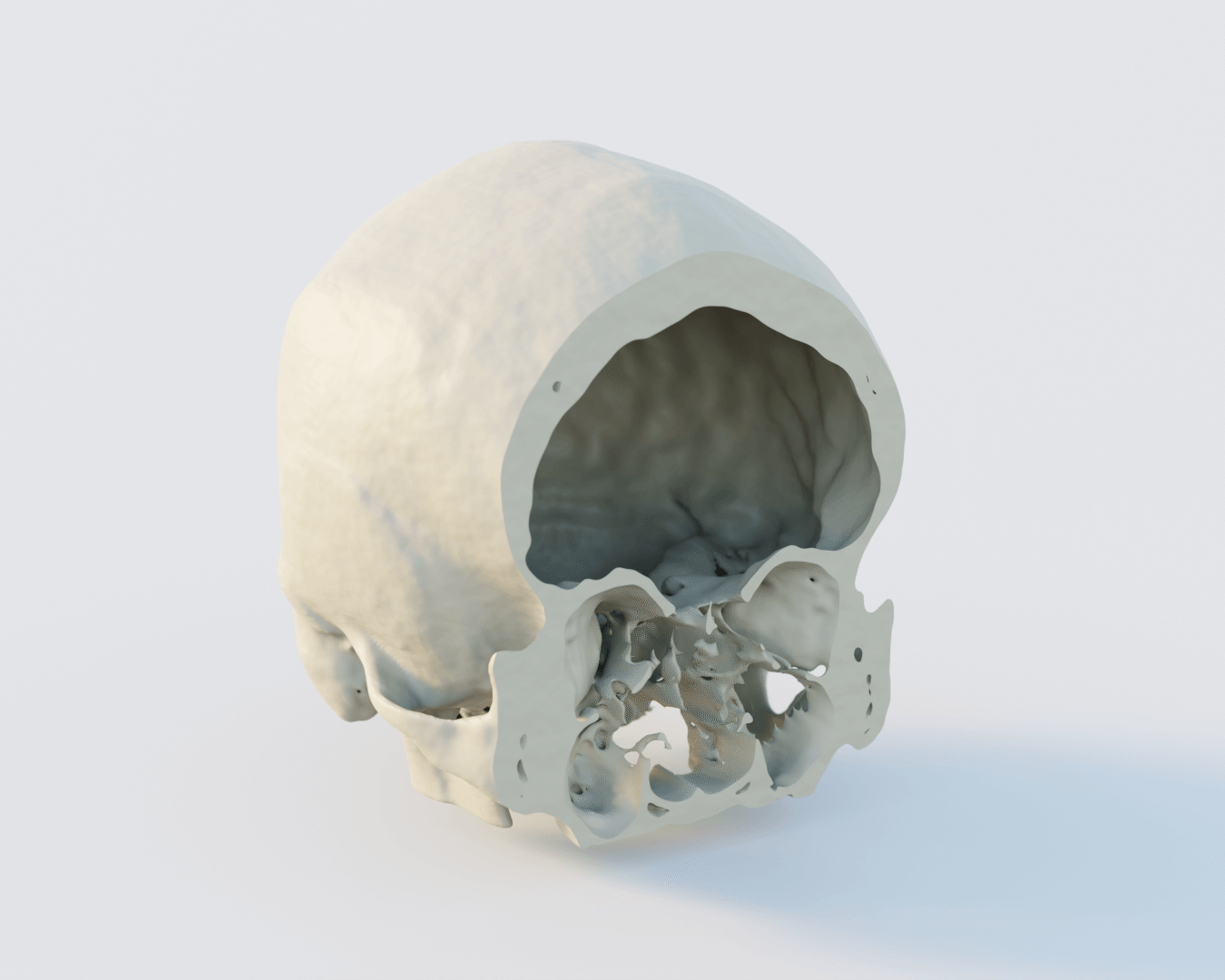
When the Implant Fails, We Reconstruct Exactly Why — From the Bone That Wasn't There to the Sinus That Was Perforated.
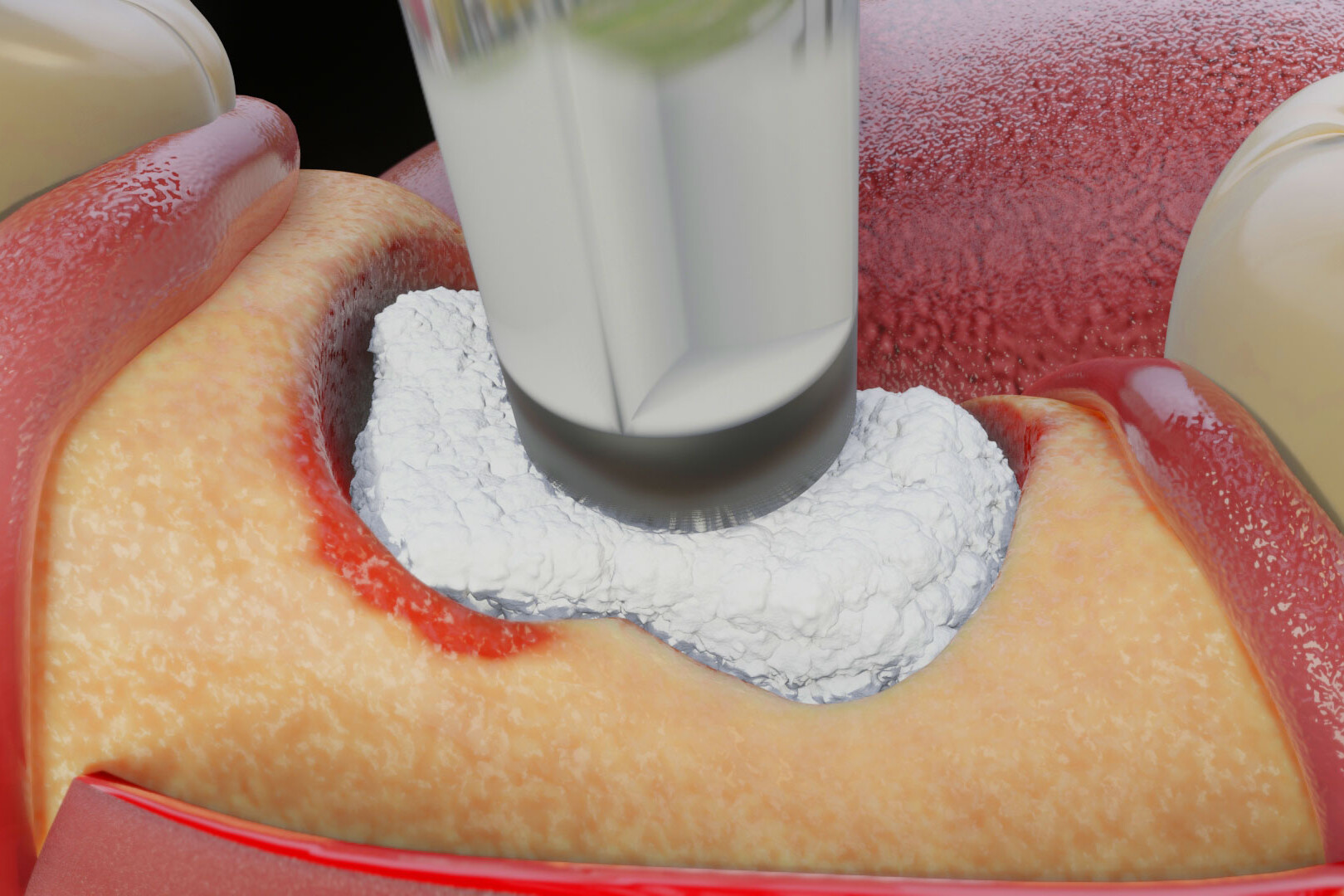
Implant failure and bone graft complication cases require a clinician who understands the biological prerequisites for osseointegration, the surgical technique required to achieve it, and the specific ways in which each can go wrong. Dr. Ho brings that direct clinical knowledge to every reconstruction — building exhibits that show not just that the implant failed, but why it was foreseeable that it would. Patient-Specific Modeling We build every reconstruction from your client's actual CBCT data — not stock dental anatomy. Bone density, ridge width, sinus proximity, root morphology, and existing pathology are all patient-specific — so the jury is looking at your client's anatomy, not a generic jaw, when your expert explains why the implant placement was negligent. Hounsfield-Validated Segmentation Cortical bone, cancellous bone, the inferior alveolar canal, the maxillary sinus floor, and metallic restorations are all individually segmented using Hounsfield Unit thresholding applied to the raw CBCT data — ensuring the 3D exhibit is a mathematically precise digital twin of your client's anatomy at the time of the procedure. Sinus Perforation & Graft Failure 3D reconstruction of maxillary sinus floor perforation, graft displacement, and subsequent sinusitis or infection — derived from pre- and post-operative CBCT imaging. The progression from the procedural error to the clinical consequence is animated in a single exhibit so causation is visually established without requiring the jury to understand the anatomy independently.
Orthognathic Surgery, TMJ & Catastrophic Facial Trauma
Beyond the Dental Chair — Maxillofacial Surgery, Joint Dysfunction, and Facial Fracture Cases.
Dental malpractice is one category of maxillofacial litigation. Orthognathic surgery complications, TMJ injury, and catastrophic facial trauma from motor vehicle collisions, assault, or falls are equally complex — and equally dependent on a clinician who understands the anatomy at the level of surgical detail. We reconstruct all of them. Orthognathic Surgery Complications Reconstruction of corrective jaw surgery complications — malocclusion, nerve damage, condylar resorption, and plate or screw malposition — using pre- and post-operative CBCT data. Side-by-side comparison of the planned surgical outcome against the actual anatomical result shows the jury exactly where the surgical execution departed from the plan. TMJ Injury & Dysfunction 3D reconstruction of temporomandibular joint disc displacement, condylar fracture, and degenerative joint changes derived from MRI and CBCT imaging — showing the structural basis for your client's chronic pain, restricted range of motion, and permanent joint dysfunction in a visual that connects the injury mechanism to the documented clinical findings. Catastrophic Facial Fractures & Trauma Hounsfield Unit-validated 3D reconstruction of mandibular fractures, midface fractures, orbital floor blowout injuries, and zygomaticomaxillary complex fractures from your client's CT data — showing the full fracture pattern, fragment displacement, and proximity to critical neurovascular structures in a single navigable exhibit your expert can use from deposition through trial.
Every Animation Is Built From Your Actual Case Records — Not Generic Templates.
Unlike generic animations, our demonstratives are reconstructed from the actual clinical record.
Operative Reports
Step-by-step surgical reconstructions from case documentation.
CT & MRI Imaging
Accurate, DICOM-derived 3D reconstructions of patient anatomy and surgical outcomes.
Expert Testimony
Every animation is developed in collaboration with your retained experts and evolves alongside their opinions.
Medical Literature
Science-backed visualizations grounded in peer-reviewed evidence.
Dedicated Medical Experts For Every Case
Dr. Kevin Ho and his own team of medical experts collaborates directly with your experts for scientifically defensible, strategically aligned medical animations.
Technical Alignment
Every visual element is reviewed against expert reports, deposition testimony, imaging findings, and evolving case facts.
Built on Defensible Science
Animations are built using transparent reconstruction techniques that experts can confidently explain and defend.
Litigation-Focused Collaboration
We help translate highly technical medical concepts into clear visual narratives that resonate with judges, mediators, and juries.
We Stay With Your Case From First Filing to Final Verdict.
Medical negligence cases take years. Expert opinions evolve. New imaging comes in. The case theory shifts. We stay engaged for the full life of the case — refining, updating, and adapting your visual evidence at every stage.
Evolving Forensic Models
As new records, imaging, or expert findings emerge, we update the master 3D models to reflect the most current picture of the injury. Your animation never becomes a liability because it was built too early.
Ongoing Litigation & Deposition Support
We build animations to support long-term litigation — not a single courtroom moment. Demonstratives are adapted through discovery, expert depositions, mediation, and trial, keeping testimony consistent from beginning to end.
The Scientific Credibility Your Opposing Experts Will Recognize
Our work is published by the same institutions cited in medical literature and expert reports. That rigor is what makes our animations defensible — not just persuasive.








Why Top Law Firms Partner with Trial Graphics 360
Unmatched experience and clarity for your case's legal animations.
$100M+
Increased settlement value in high-stakes litigation.
Medically-Trained Animators
Board-certified specialists and former UBC professors ensuring medical accuracy for complex litigation.
Scientifically Published
Harvard, Stanford, and pharma-published expertise giving your case a distinct litigation edge.
Long Term Case Support
End-to-end case support, refining visuals as evidence evolves.
Common Questions About Dental & Maxillofacial Animation
Dr. Kevin Ho is a practicing dentist and clinic owner. He reads CBCT imaging in clinical practice, performs the procedures at issue in these cases, and brings direct clinical judgment to every reconstruction — not just anatomical illustration from reference materials. When he identifies a nerve proximity violation in a CBCT scan, he is making the same clinical assessment a treating dentist should have made before proceeding with the procedure. That distinction is significant in court.
Pre-operative CBCT imaging is the most critical exhibit in a dental nerve injury case — it shows what the clinician should have seen before proceeding. Post-operative CBCT or panoramic imaging documents the implant or instrument position after the fact. We work with whatever imaging is available and can advise on what additional records to request in discovery to build the strongest possible reconstruction.
Yes — and the absence of pre-operative CBCT imaging is often itself evidence of a standard-of-care violation. We can reconstruct the post-operative anatomy from available imaging, derive the pre-operative anatomy from the clinical record, and build an exhibit that shows both what the imaging would have revealed had it been taken and what the defendant proceeded without knowing as a result.
Yes. Our methodology is fully documented — CBCT segmentation parameters, Hounsfield Unit thresholding values, nerve canal identification protocol, and peer-reviewed implantology literature citations are all recorded. Dr. Ho can provide a complete methodology report and your expert can defend every frame from the stand against opposing dental and oral surgery expert challenge.
Most dental and maxillofacial animations are completed in 3–6 weeks depending on the complexity of the surgical history and the volume of CBCT imaging data. Rush delivery is available — send us your mediation or trial date and we will confirm availability the same day.